
Canine Cruciate Ligament Rupture

What is the cranial cruciate ligament?
Additionally, there are multiple ligaments (tough bands of tissue that attach the bones to other bones) within the knee joint, which help to provide stability during movement. Two of these ligaments, that connect the femur and tibia, are the ‘cruciate’ ligaments, so-called as they cross over each other. In humans, these are known as the ‘anterior’ and ‘posterior’ cruciate ligaments, but in dogs, the same ligaments are named the ‘cranial’ and ‘caudal’ ligaments.
The main function of the cruciate ligaments is to prevent the tibia from sliding backwards and forwards in relation to the femur. This is important to ensure normal, pain-free function of the knee joint. The cranial cruciate ligament (CCL) prevents the tibia from sliding forwards in relation to the femur. The caudal or posterior cruciate ligament is only very rarely damaged due to its more robust nature and the different forces which act on it.
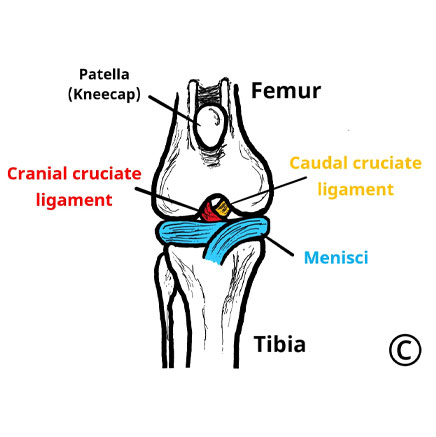
Image copyright of Rebecca Jones
Image of the canine knee joint from the front,
showing the position of the cruciate ligaments and menisci
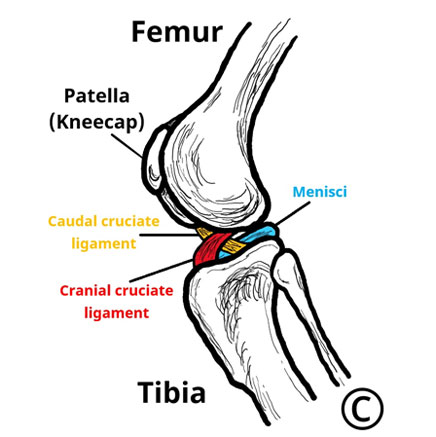
Image copyright of Rebecca Jones
showing the position of the cruciate ligaments and menisci
What causes cranial cruciate ligament disease in dogs?
In young people, rupture of the anterior cruciate ligament (the equivalent of the CCL) is most often the result of a sports injury (e.g. football or skiing). Excessive forces through the otherwise normal ligament overwhelm the ligament and it snaps suddenly.
In dogs and older people, the situation is usually very different. Instead, the CCL slowly degenerates and weakens over time (like a fraying rope) until it is unable to withstand the forces of normal movement. We do not know the exact cause of this degeneration, but genetics likely play a role, as certain breeds are more commonly affected, though it is seen in almost every breed and crossbreeds. Other factors, such as being overweight, the shape of the leg and hormones also influence whether a dog will be affected.
Approximately 40-50% of dogs affected by CCL disease will be affected in both knees, though the ligaments often rupture at different times.
Why is cranial cruciate ligament disease a problem?
When a dog has CCL disease, the fibres of the ligament gradually stretch and tear. This, as well as the subsequent instability, triggers inflammation (swelling) in the joint, which causes pain and osteoarthritis. As a result, in early disease, dogs may show signs of mild, intermittent, or progressive lameness which tends to be worse following exercise, though in some dogs the first sign is sudden, severe lameness. Even if the lameness occurs suddenly in most cases, the ligament will have been abnormal even without any initial signs of lameness.
At a critical point, the CCL becomes too weak to stop the shinbone and thighbone sliding relative to each other, which enables the shinbone to shift forwards every time the dog takes a step. This may happen after minor trauma or particularly boisterous play, although most often the underlying disease process has been present for some time. This abnormal movement can be very painful and can damage other important structures of the joint.
How is cranial cruciate ligament disease treated?
Given this, surgery is recommended for most patients. Surgery aims to stabilise the knee to reduce pain and ongoing damage to other structures within the joint. This is expected to result in a faster recovery and better function in the long term.
How is cranial cruciate ligament disease treated?
1. Intra-articular stabilisation
This technique aims to place an artificial or natural grafted ligament within the joint to mimic the action of the CCL.
2. Extra-capsular stabilisation
This technique involves the placement of a suture outside the joint capsule to anchor the tibia and femur together and eliminate the sliding motion during walking. Ultimately, this suture is expected to weaken, but over time the body naturally forms scar tissue near this suture which will take over the action of the suture once it fails. The Extracapsular Lateral Suture Stabilisation (ELSS) is the most common example.
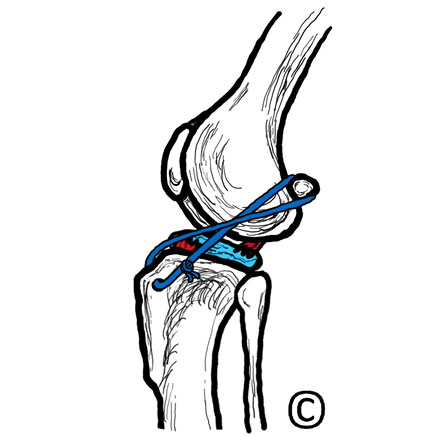
Image copyright of Rebecca Jones
Image of the canine knee joint showing an extra-capsular repair.
3. Osteotomy procedures
The top of the shinbone, or tibial plateau, in dogs generally slopes backwards. This predisposes the thighbone (femur) to slip backwards and push the shinbone (tibia) forwards when the dog bears weight, with steeper angles increasing this effect. The muscles attached to the bones of the knee joint exacerbate this. In normal knee joints, the CCL resists this movement but once it has ruptured the bones slide against each other, due both to the shape of the bones and the pull of the surrounding muscles.
Osteotomy procedures aim to restore joint stability by altering the biomechanics of the joint, effectively removing the need for an intact cranial cruciate ligament, either by flattening the top of the tibia (such as with CCWO, CBLO and TPLO procedures) or by altering the muscular forces acting on the joint to prevent them from pulling the tibia forwards (such as with the TTA procedure).
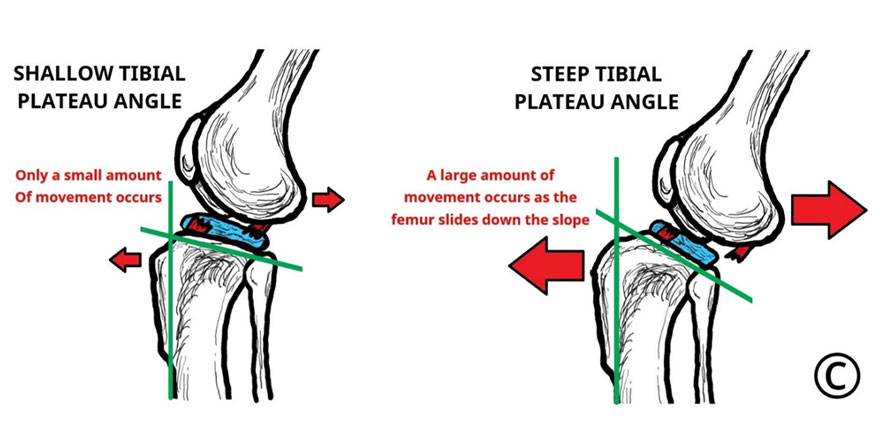
Image copyright of Rebecca Jones
Image of the canine knee joint to show the different forces acting on the joint which are affected by the slope of the shin bone
Contibutors
Authors: Dr Catrina Pennington BVM&S MRCVS and Dr Rebecca Jones BVM BVS MRCVS
Catrina graduated from the University of Edinburgh in 2014. After two and a half years in small animal, first opinion practice she completed a rotating internship followed by a period as a surgical registrar at Chestergates Veterinary Specialist. She returned to Edinburgh University in 2018, completing an internship in Soft Tissue and Oncological surgery before starting her current position as a Clinical Fellow in Small Animal Surgery at the Royal Veterinary College.
Editor: RCVS Knowledge Communications Team
Reviewer: Mark Morton BVSc DSAS(Orth) MRCVS